
FINDING TREATMENT
FAMILY EXPERIENCE IN FINDING TREATMENT
Families quite often feel helpless while watching their loved one suffer with BPD and they are frantic to ensure their loved one’s safety and well-being. They have great faith in the healing ability of professionals and work very hard trying to motivate and engage their loved one to go into therapy, any type of therapy. Unfortunately, non-evidence based general treatments have been shown to be ineffective for BPD and therefore turn out to be a waste of emotional effort, time and money. At worst, they are iatrogenic. The person with BPD will drop out of therapy leaving them feeling as if they have, once again, “failed”, no treatment can help them and they wind up feeling more hopeless than before. This conclusion is based on experience working with families as well as from people with BPD who participated in TARA’s, “Get The Facts BPD”, Psychoeducation classes. Family members trust the professional and often blame their loved one for not “trying hard enough” while not considering the responsibility of the therapist to develop a connection with the client to avoid termination of therapy. Once the client ends therapy the relationship between the individual and the family is jeopardized. Both parties lose confidence in mental health services. After such an experience, why turn towards another treatment in the future?
WHY SO LITTLE RESEARCH IS DONE ON BPD
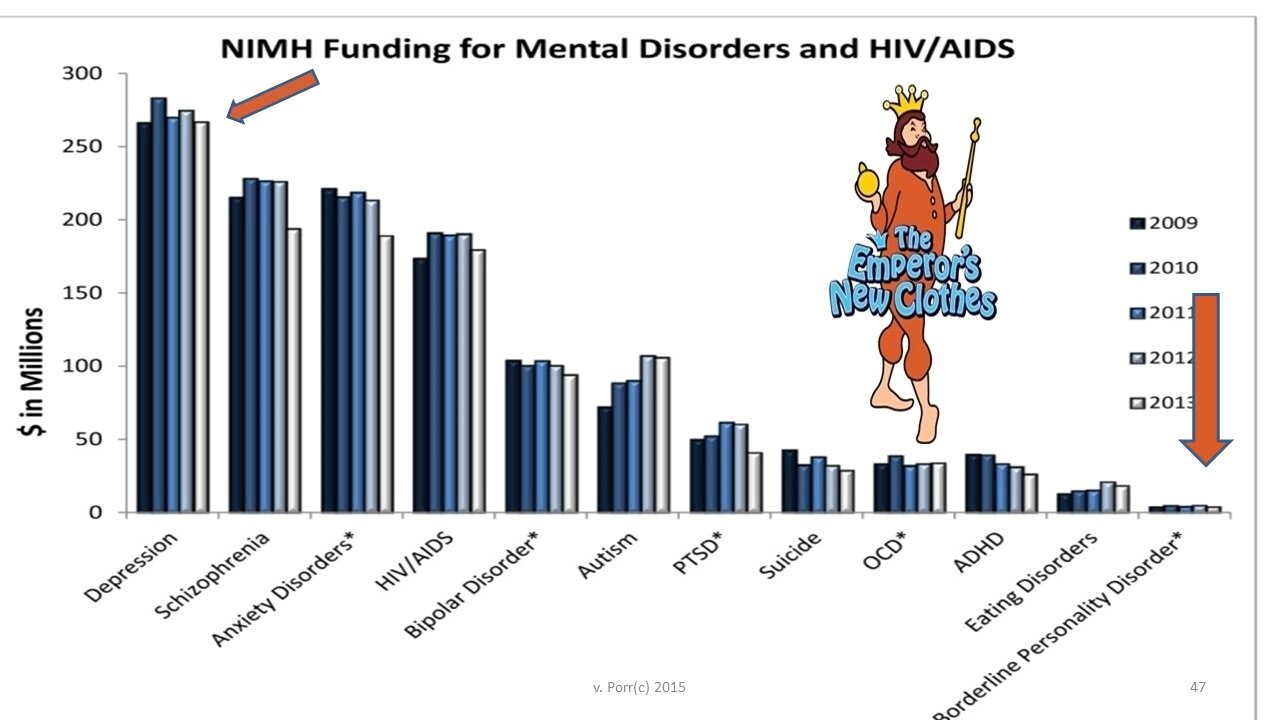
RESEARCH & TREATMENT FUNDING: Psychiatric research and treatment funding usually comes from the Federal Government through the National Institute of Mental Health (NiMH). Prevalency rates of disorders and the advocacy efforts on behalf of a specific disorder may be the major factors influencing decision making at NIMH as to who gets research, treatment or educational funding. Of course, if a member of the Senate or the House, especially a member on the committees that fund NIMH, has a particular interest in a disorder, you can be sure it will receive more attention This same system holds true at State and local levels
STIGMA: Doctors and the psychiatric community continuously trivialize BPD or deem these patients non-treatable, often refusing to treat them. A national educational campaign to raise awareness of the latest research findings on etioiogy, genetic studies, neurobiological findings and treatment options for BPD is desperately needed in order to reframe BPD as the severe, chronic and costly mental illness that it actually is. People with BPD can get better; outcome studies are available demonstrating how people with BPD improve with appropriate treatment. (Linehan). Appropriate and effective treatment is not available in most communities.
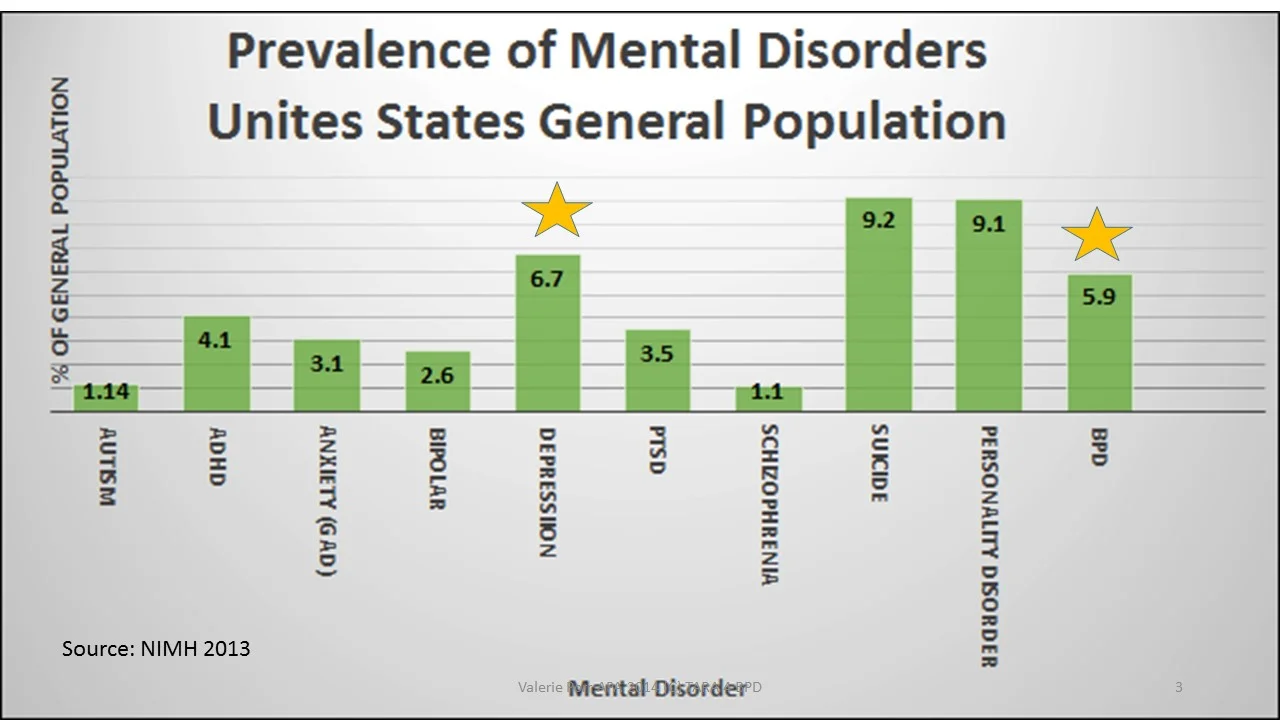
BPD affects approximately 18 million people however treatment is not available in many locations and BPD receives the least amount of research funding of any mental illness.
PUBLIC AWARENESS: The public is by and large unaware of BPD. Scant media attention has been paid to this disorder. BPD does not as yet have a public figure as a spokesperson.
ADVOCACY: Families of people with BPD receive little or no help in understanding BFD or in coping with their loved ones with this disorder. There are very few support groups available for family members or for people with BPD. In short, BPD is the most maligned, misunderstood and mistreated of all mental illnesses.
CHILDREN & ADOLESCENTS: Clinicians are reluctant to diagnosis BPD in adolescents or younger children. Failure to diagnose when symptoms first appear leads to development of maladaptive coping methods such as drug abuse, alcoholism, unsafe sex and other disorders of impulsivity. There is very little treatment available, to date, for adolescents.
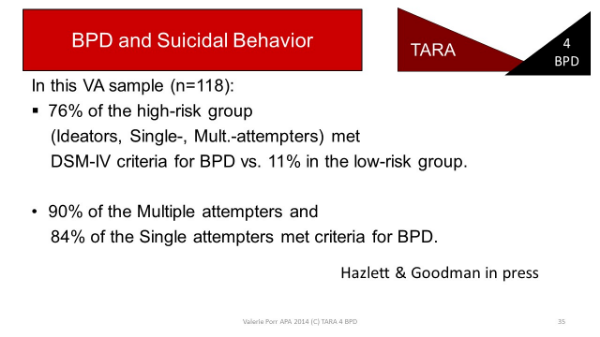
SURGEON GENERAL'S REPORT ON SUlCIDE: The Surgeon General has launched an ANTI-SUICIDE crusade that focuses on the Public Health implications of suicide, stressing suicide prevention. This program excludes consideration of BPD in its advocacy for suicide prevention despite the fact that the suicide rate for BPD is greater than the combined total of suicides from schizophrenia and bi-polar disorder. BPD suicides are usually impulsive in nature and are distinct enough to merit attention. Omission from this ANTI-SUICIDE effort flies in the face of the research findings regarding violent suicides Suicide is not just about depression.
IS THERE ANY WONDER WHY PEOPLE WITH BPD DON T GET BETTER? UP TO NOW, A NATIONAL ORGANIZATION FOCUSED ON ADVOCACY FOR THE BPD POPULATION HAS NOT EXISTED. TARA APD IS THE FIRST AND ONLY NATIONAL NOT FOR PROFIT ORGANIZATION ACTIVELY WORKING TO CHANGE THE PROGNOSIS AND BRING HOPE TO PECPLE SUFFERING WITH BPD & THEIR LOVED ONES.